Early orthodontics in children with mixed dentition
For some Orthodontic problems, early intervention by the Orthodontist is necessary. The word “early” means that treatment is provided while the patient is in a period of mixed dentition (he also has permanent teeth in the mouth). Early intervention does not necessarily exclude the need for future treatment, but guarantees the simplification of any future problem (e.g. avoidance of permanent tooth extraction, avoidance of skeletal asymmetry, etc.).
The following cases require early intervention:
- Sagittal skeletal discrepancies
Mandibular prognathism
When the lower jaw is anterior in relation to the jaw
![]()
Mandibular retrognathism
When the lower jaw is far behind in relation to the upper jaw

Causes
The main causes of crossbite occlusion is heredity and the environment.
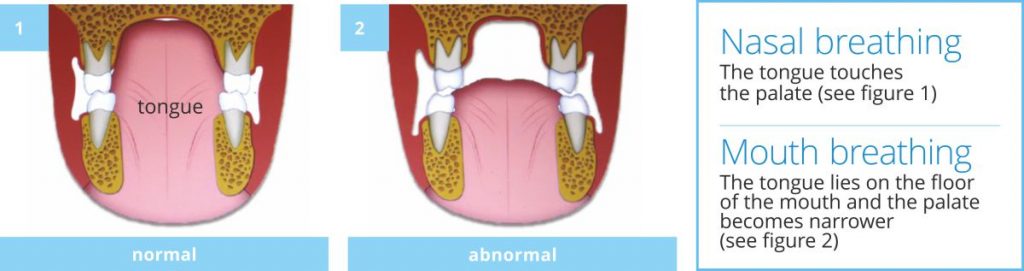
The environmental causes involve prolonged use of pacifiers or thumb or finger sucking and mouth breathing. The finger or the pacifier forces the tongue downwards and away from the palate and it results to narrowing of the palate since the tongue support is lost. This narrowing causes crossbite.
Mouth breathing in a similar way causes crossbite since the tongue lies on the floor of the mouth and away from the palate.
When is the best age for the treatment of crossbite occlusion?
According to research, the best age for the correction of this problem is the age of 6-7 since at this stage we achieve pure skeletal correction which has a more stable and long lasting result. Correction of crossbite occlusion may also be done at an older age (up to 16-17 years old) but many times the results are not pure skeletal expansion and as the age increases the relapse tendency increases too.
This happens in older ages because the mid palatal suture, which is the area where the two bones of the hard palate connect to each other, becomes more ossified thus increasing its resistance to expansion.
How do we correct crossbite?
Special fixed intraoral appliances are placed in the upper jaw applying orthopedic forces that cause the mid palatal suture to open. The upper jaw becomes wider and the upper teeth occlude correctly (outside) the lower teeth. This correction will lead to the right occlusion, preventing this way the development of any facial asymmetry thus eliminating the need of any future surgical intervention.

- Mouth breathing
It is a serious problem if the child continues to breathe through his mouth instead of his nose while growing up. Mouth breathing is pathologic and under no circumstances should be considered physiological. Usually, it is due to enlarged tonsils and adenoids, allergic rhinitis or deviated nasal septum.
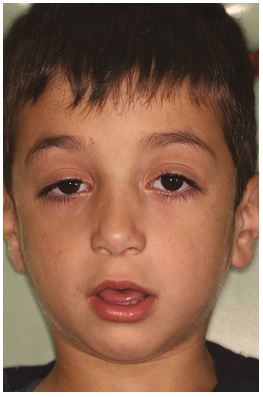
Very often mouth breathing remains unnoticed from the parents and the Pediatrician. Chronic mouth breathing affects negatively the growth of the face. It leads to a characteristic type of face known as adenoid face (see image).
This happens when the tongue sinks into the lower jaw in order to open the upper airway (image 2), instead of touching the palate (image 1). This results in:
- An opening between the upper and lower front teeth (openbite)
- Narrowing of the upper jaw since it is not supported by the tongue and it develops into crossbite (image 1)
Apart from crossbite, chronic mouth breathing in children can cause insufficient brain oxygenation which leads to lethargy, tired look like face, dark circles under the eyes, constant fatigue and poor performance in the class and in sports. These children also have a poor quality of sleep due to this breathing disorder. This condition causes a reduction of the growth hormone which is mainly produced and released during sleep from hypophyses, a gland that is located in the brain, which eventually leads to short statue children. Once normal breathing is established in the children, all the above symptoms disappear and normal growth reiterates. The earlier the correction the better the results are.
It is good to keep in mind that no Orthodontic problem can have a stable result if the child continues to breathe through their mouth.
- Crowding of the teeth
Early intervention can also help in the causes of severe lack of space leading to the eruption of permanent teeth (Guidance of Eruption) in their correct position in the jaw. This can be done by premature extraction or slicing of the primary teeth (image 2) which eventually creates the space to alleviate the crowding, reducing this way the intensity and severity of the problem (e.g. avoid extracting permanent teeth) and in some instances it completely eliminates the need of any future Orthodontic treatment.
If we do not intervene, the teeth erupt ectopically, meaning that they erupt at a more forward or at a lingual position, (image 1,3,5) or they are rotated at a high degree in order for them to take some place in the jaw.
Teeth that erupt this way do not have a good quality of bone and gums to surround their roots, and as a result the gums recede since they present no resistance to masticatory forces and eventually the roots become denuded (image 1).
Even after Orthodontic treatment, such gums cannot go back to the correct position and these teeth remain vulnerable to periodontal problems (image 6).
It is the condition where the upper and lower anterior teeth cannot come into contact. This is due to the skeletal discrepancy or to a deleterious habit such as finger sucking or prolonged use of pacifiers or to chronic mouth breathing (image 2, 5).
If open bite is due to finger sucking or tongue thrusting, then an appliance should be used to stop this habit (image 4) and most of the times the open bite will self-correct (image 6)

If the child continues the finger sucking habit after the age of 4, every time they swallow, the tongue will thrust in between the teeth, maintaining and many times increasing the open bite. This tongue thrust while swallowing will eventually be registered in the brain and will develop into a habit making its discontinuation very difficult (image 3) since on an average, every human being swallows 1000 per day.
If the cause of open bite is mouth breathing, then again the cause should be treated so as to achieve self-correction or a successful and stable outcome of the orthodontic treatment. Failure to provide treatment during the growth period, the open bite may develop into a skeletal problem and the therapy will be a combination of surgery and Orthodontic treatment
